-
Call Now
1800-102-2727


Urine Formation, Practice Problems and FAQs
A clean body is always healthy. External cleanliness can be achieved through taking a bath everyday and cleaning the body parts using soap and water. Is external cleanliness enough to maintain a clean body? Absolutely no. The body should be clean internally too.
There are many types of waste products like metabolic wastes, undigested food materials etc. present inside our body. All these wastes are eliminated from our body through the same path? The answer is no!! The undigested food is eliminated through the anus as faeces. This process is called egestion. Now what about the metabolic waste products? These waste products can be nitrogenous (urine and sweat) or gaseous (CO2). This is eliminated through a process called excretion. Hence respiration is also a part of excretion.
The process of excretion differs in animals. In the human excretory system, we have a pair of kidneys, a pair of ureters, a urinary bladder and a urethra. So in what form do we excrete our nitrogenous metabolic wastes? In the form of urine which contains urea. Hence we are called ureotelic animals. How urine is formed then? What are the processes behind it? Let’s discuss more about the formation of urine in this article.
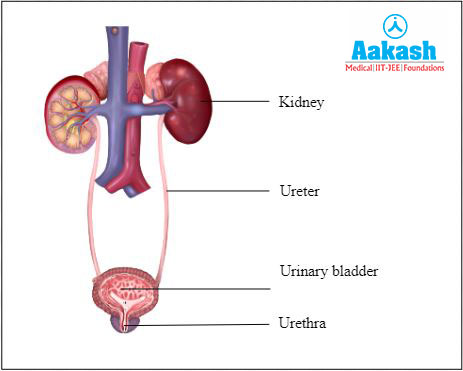
Fig: Human excretory system
Table of contents
- Urine
- Urine formation
- Glomerular filtration rate
- Counter current mechanism for the concentration of nephric filtrate
- Practice Problems
- FAQs
Urine
A fluid produced by kidneys that contains wastes and excess materials that are excreted through urethra is called urine. Under normal conditions an adult man may excrete 1.2 to 1.5 litres of urine per day.
Urine is transparent and pale yellow in colour, due to the presence of pigment called urochrome. It has an acidic pH (pH 6.0). It has higher osmotic pressure than blood plasma, hence it is hypertonic. It also has a characteristic odour.
Fig: Urine
Composition of urine
It consists of 95% water and 5% of other organic and inorganic substances. Organic substances include nitrogenous compounds (urea, uric acid, creatinine and hippuric acid) and non nitrogenous compounds (vitamin C, oxalic acid, phenolic substances and traces of glucose). The principal component of human urine is urea. Inorganic substances include ammonia and mineral salts (chlorides, sulphates, potassium, calcium etc.). The principal mineral salt of urine is sodium chloride. Urine can also contain pigments, drugs and other unwanted materials from our body.
Urine formation
The process of formation of urine is called uropoiesis. The formation of urine in each individual depends upon the following factors:
- Fluid intake
- Diet
- Level of physical activity
- Environmental temperature
Urine output is more if there is excessive fluid intake and low environmental temperature. Diuretic substances like tea, coffee and alcohol also increase the urine output.
Site of urine formation
Kidneys are the site of urine formation. They purify the blood and it is done by the structural and functional units of the kidney called the nephrons. Each nephron has two parts and they are as follows:
- Renal tubules
- Glomerulus
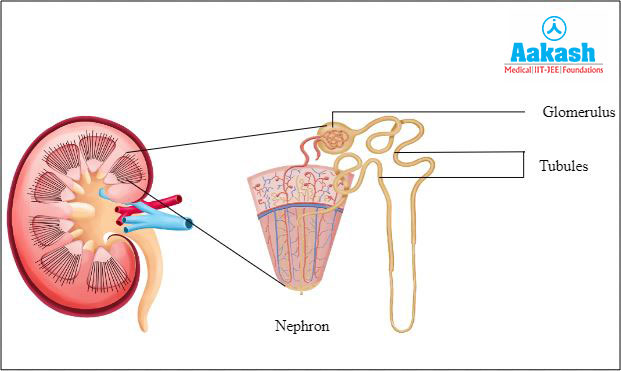
Fig: Structure of nephron
Renal tubules
There is a double walled cup-like structure called Bowman’s capsule at the beginning of renal tubules. Glomerulus and the Bowman’s capsule are together called the Malpighian body or renal corpuscle.
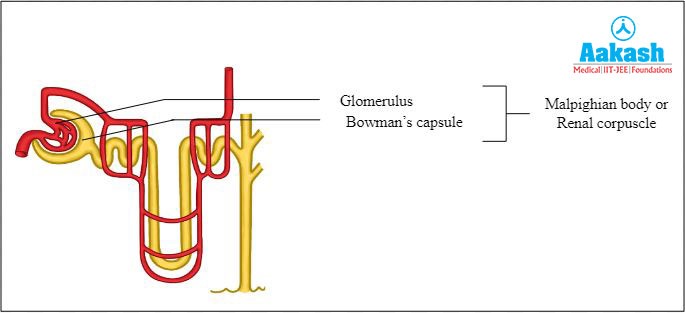
Fig: Malphigian body
The renal tubules continue to form the proximal convoluted tubule (PCT), which is a highly coiled network. The next part of the tubule is the Henle’s loop, which has a hairpin shape and possesses an ascending and descending limb. The continuation of the ascending limb is called distal convoluted tubule (DCT), which is also another highly coiled tubular region. The next part of a nephron is the collecting duct, which is a straight tube.
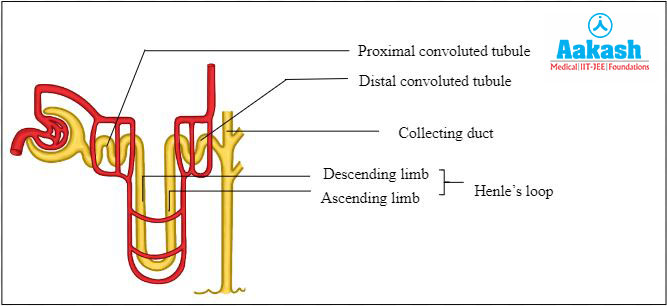
Fig: Parts of renal tubules
Glomerulus
Glomerulus is a tuft of capillaries which resembles a ball of thread. It is formed by the afferent arteriole, which is a fine branch of the renal artery. An efferent arteriole carries the blood from the glomerulus. The efferent arteriole emerging from the glomerulus forms a fine capillary network around the renal tubule and it is called the peritubular capillaries. A minute vessel of this network runs parallel to the Henle’s loop is called vasa recta, which is ‘U’ shaped.

Fig: Glomerulus
Steps of urine formation
The various processes involved in the formation of urine occur at different parts of the nephron. There are three major steps for the formation of urine and they are as follows:
- Ultrafiltration
- Tubular reabsorption
- Tubular secretion
Ultrafiltration
The process of ultrafiltration is done by Bowman’s capsule. The filtration of blood happens when blood passes through the glomerular capillaries. Afferent arterioles bring blood in and efferent arterioles take blood out of the glomerulus. The glomerular capillaries are narrower than afferent arterioles. Ultra filtration happens when the pressure in the glomerular capillaries becomes very high.

Fig: Ultrafiltration
Filtration membrane
The blood pressure in the capillaries of glomerulus causes filtration of blood through the below mentioned three layers as follows:
- The epithelial layer of the Bowman’s capsule.
- The endothelial layer of the glomerular blood vessels.
- The basement membrane which is present between the above mentioned two layers.
The epithelial cells of Bowman’s capsule are called podocytes. They are arranged in an intricate manner. These cells possess foot-like processes called pedicels and leave some spaces. Such spaces are called slit pores or filtration slits.
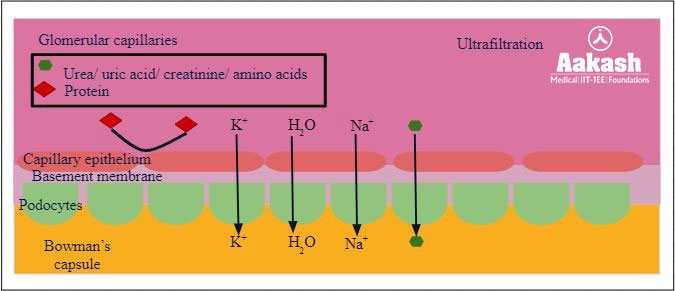
Fig: Process of ultrafiltration
Water and all substances dissolved in the blood plasma (except blood cells, colloids and certain plasma proteins) gets filtered into the Bowman’s capsule from the glomerular capillaries. Hence ultrafiltration is also called glomerular filtration. The filtrate fluid is called nephric filtrate, glomerular filtrate or ultrafiltrate. Now the filtrate is in Bowman’s capsule.
Glomerular filtration rate (GFR)
Filtrate formed by the kidneys per minute is known as glomerular filtration rate or GFR. It is 125 ml/min (approx.) which is 180 litres per day for a normal human. But we do not release 180 litres of urine everyday. Only around 1.5 litres of urine is released per day. This suggests that nearly 99 percent of the filtrate has to be reabsorbed by the renal tubules. This process is called reabsorption.
GIF: Path of blood, filtrate and urine
Tubular reabsorption
The filtrate from the Bowman’s capsule has to pass into the proximal convoluted tubules, Henle’s loop and distal convoluted tubules to reach the collecting duct. In this process the composition, osmotic pressure and pH of the filtrate changes. This is due to the reabsorption of water and many solutes from the filtrate in the tubules. This reabsorption of useful substrates from the nephric filtrate into the blood capillaries is called tubular reabsorption or selective reabsorption.
The reabsorption of the following materials are achieved through the below mentioned processes:
- Diffusion - K+, Ca2+ and Mg2+
- Facilitated diffusion - K+, Cl-, HCO3-, PO43-, amino acids, glucose, fructose etc.
- Active transport - Na+
- Cotransport - K+, Cl-, Ca2+, Mg2+, HCO3-, amino acids, glucose, fructose, lactate and citrate
- Osmosis - Water
Regions of tubular reabsorption
The process of reabsorption happens in five major parts of the nephron. They are as follows:
- Proximal convoluted tubule (PCT)
- Henle’s loop
- Distal convoluted tubule (DCT)
- Collecting tubule
- Collecting duct
Reabsorption in proximal convoluted tubule (PCT)
The epithelial cells of PCT possess numerous mitochondria and microvilli. This is a specialisation for reabsorption in PCT. Most of the essential nutrients, and 70 - 80 percent of water and electrolytes are reabsorbed by PCT.
The reabsorption of following components from the filtrate happens at PCT:
- Entire glucose
- Amino acids
- Inorganic ions (Na+, K+ and Cl-)
- Water
- Urea

Fig: Reabsorption in proximal convoluted tubule (PCT)
Reabsorption in Henle’s loop
Minimum amount of reabsorption happens at Henle’s loop. Henle’s loop has a descending limb, and an ascending limb. The reabsorption process is different in both the loops. The descending limb of the loop of Henle is considered permeable to water but it is impermeable to electrolytes due to lack of transporters. The ascending limb is considered impermeable to water but it allows the transport of electrolytes passively or actively, because they lack aquaporins.
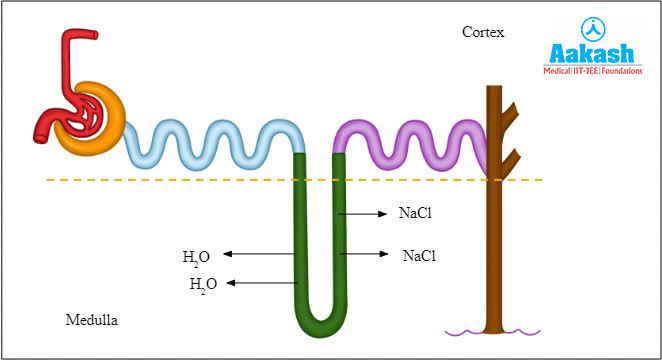
Fig: Reabsorption in Henle’s loop
Descending limb
The descending limb has an upper thick segment and lower thin segment. Upper segment is located in the cortex of the kidney and it is impermeable to ions, urea and water. The major function of this part is to transfer the isotonic solution from the PCT to the narrow segment.
The thin segment is permeable to water and it is present in the outer and inner medulla of the kidney. The interstitial fluid surrounding the limb has higher concentration of NaCl and urea. So the osmotic pressure of the outer fluid is more than the inner fluid of the descending limb. Hence the water moves out from the filtrate of the lower thin segment of the descending limb to the interstitial fluid through osmosis. When water content refuses in the filtrate, it becomes hypertonic.
Ascending limb
The hypertonic filtrate from the descending limb enters the ascending limb. It also has a lower thin segment which is in the inner medulla and an upper thick segment which is in the outer medulla and cortex. Lower segment is permeable to ions (Na+, K+, Cl-) and urea. Since the outer interstitial fluid has high concentration of urea, the urea enters the lower segment by diffusion. But the concentration of ions is more inside the limb, so the ions move out of the limb by diffusion.
Now the filtrate moves from the thin segment to the thick segment of the ascending limb. The active transportation of NaCl from filtrate to the interstitial fluid in the medulla of the kidney happens here. As a result the osmolarity of the inner medulla of the kidney increases. But the filtrate inside the limb becomes hypotonic to the blood plasma due to loss of NaCl. This hypotonic filtrate then passes into DCT.
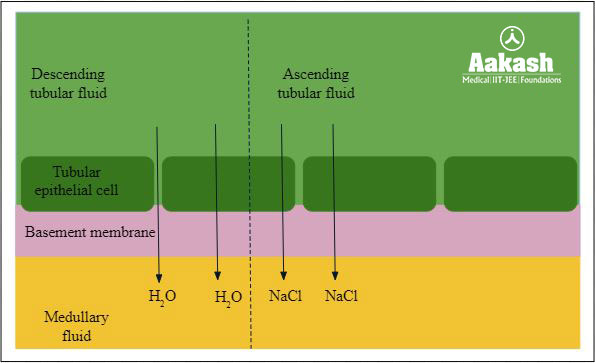
Fig: Reabsorption in the descending and ascending limb of Henle’s loop
Reabsorption in distal convoluted tubule (DCT)
Reabsorption of water, Na+ ions, HCO3- and amino acids occurs at DCT.
Reabsorption of water
ADH is released by the posterior pituitary, when the water in blood plasma goes down. This will increase the permeability of the distal convoluted tubule. The water is reabsorbed from the filtrate to the interstitial fluid and highly concentrated urine in less amount is produced.
When the water level in the plasma comes to normal, the ADH secretion stops and it affects the permeability of the DCT. Hence less water is reabsorbed from filtrate. As a result diluted urine in more quantity is produced.
Reabsorption of Na+ ions
The reabsorption of sodium ions from the filtrate to the interstitial fluid occurs under the influence of aldosterone. The reabsorption of sodium results in the uptake of equivalent amounts of water.
In the absence of or less concentration of aldosterone, the DCT is impermeable to ions.
Reabsorption of HCO3- and amino acids
Reabsorption of HCO3- ions and amino acids are reabsorbed from filtrate into medullary interstitial fluid.
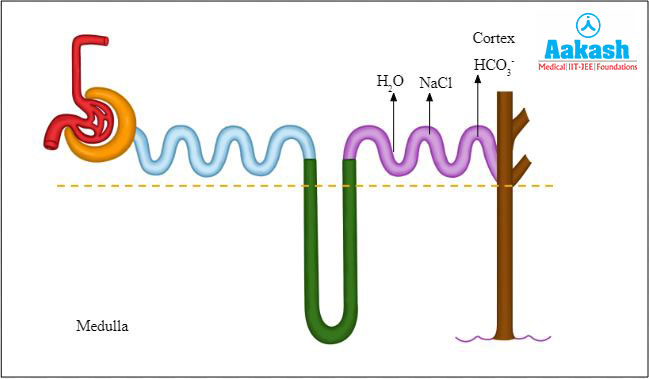
Fig: Reabsorption in DCT
Reabsorption in collecting duct
All the three types of abosoptions happening at DCT like the reabsorption of water, Na+ ions, HCO3- and amino acids also happen in the collecting tubule and collecting duct. Collecting duct is considered as a long duct that extends from the cortex part of the kidney to the medulla’s inner part. Higher amounts of water is reabsorbed from this region which results in the production of concentrated urine. This region also allows the passage of small amounts of urea to the interstitium of medulla to maintain the osmolarity.
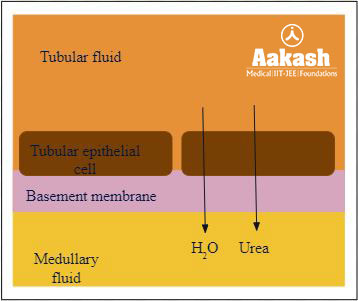
Fig: Reabsorption in collecting duct
Tubular secretion
The movement of some toxic substances from peritubular capillaries, interstitial fluid and the epithelial cells of nephrons into the glomerular filtrate is called tubular secretion. This can take place either through active or passive transport.
Those substances that secreted into the filtrate are as follows:
- The ionic balance and pH of the body fluids are maintained with the help of PCT through selective secretion of ammonia, hydrogen ions, and potassium ions into the filtrate.

Fig: Tubular secretion at PCT
- Urea enters the ascending limb of Henle’s loop.
- K+ ions are secreted into DCT and collected through active transport.
- H+ and NH4+ ions are secreted from blood to DCT through active transport.
- Creatinine, hippuric acid, para-amino hippuric acid, drugs, pigments etc. are secreted into the DCT from interstitial fluid.

Fig: Tubular secretion at DCT
- Collecting duct also plays a role in the maintenance of pH and ionic balance of blood by the selective secretion of H+ and K+ ions.
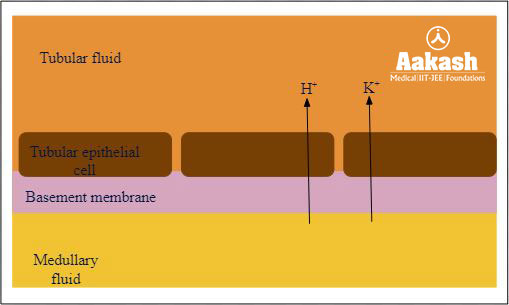
Fig: Secretion in collecting duct
Counter current mechanism for the concentration of nephric filtrate
The urine is concentrated in Henle’s loop and vasa recta. The capillary network which forms a parallel set of hairpin loops within the medulla of kidney and supplies blood to it is called vasa recta.
Blood flows in the opposite directions though the two limbs of Henle’s loop and this is same as in vasa recta. This forms a counter current pattern. This system of flowing a liquid in two limbs in opposite directions is termed as a countercurrent mechanism. The high solute concentration in the kidney medulla is maintained through this process.
Counter current mechanism in Henle’s loop
The ascending and descending limbs of Henle’s loop run parallel to each other in the medulla. The glomerular filtrate flowing through it is in the opposite direction and forms a counter current.
When the fluid passes through the ascending lymph of the Henle’s loop, the sodium ions leave the tubular fluid and re-enter the interstitial fluid. As a result the electrolyte concentration of the interstitial fluid increases, and osmolarity increases. This will draw out the water from the descending limb through osmosis. This water quickly enters the vasa recta to increase the blood volume.
Counter current mechanism in vasa recta
The blood flowing slowly through the vasa recta gives sufficient time for the diffusion of water and solutes from the filtrate into the blood. The countercurrent mechanism in the vasa recta prevents the loss of Na+ and Cl- ions from renal medulla and also helps to maintain the concentration gradient in the renal medulla. Thus they assist in concentrating urine by the loop of Henle.
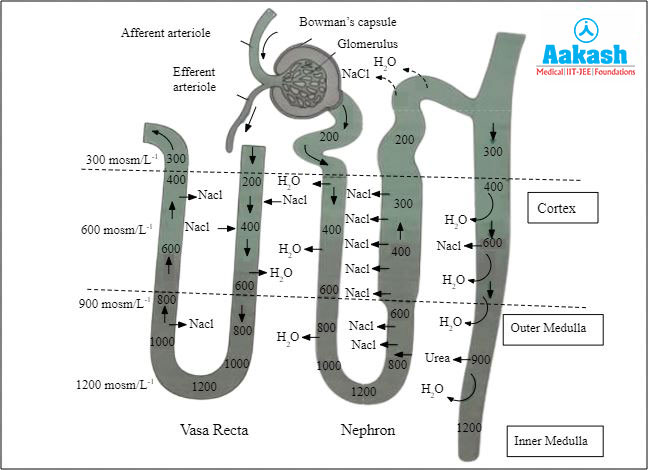
Fig: Counter current mechanism of nephric filtrate
Practice Problems
1. Which of the following is a part of renal tubule?
- Proximal convoluted tubule
- Henle’s loop
- Distal convoluted tubule
- All the above
Solution: There is a double walled cup-like structure called Bowman’s capsule at the beginning of renal tubules. Glomerulus and the Bowman’s capsule are together called the Malpighian body or renal corpuscle. The renal tubules continue to form the proximal convoluted tubule (PCT), which is a highly coiled network. The next part of the tubule is the Henle’s loop, which has a hairpin shape and possesses an ascending and descending limb. The continuation of the ascending limb is called distal convoluted tubule (DCT), which is also another highly coiled tubular region. The next part of a nephron is the collecting duct, which is a straight tube. Hence the correct option is d.
2. Which of the following is wrong about the ultrafiltration in the urine formation?
- The process of ultrafiltration is done by Bowman’s capsule
- Efferent arterioles bring blood in and afferent arterioles take blood out of the glomerulus
- Ultrafiltration is also called glomerular filtration
- The filtrate fluid is called nephric filtrate
Solution: The process of ultrafiltration is done by Bowman’s capsule. The filtration of blood happens when blood passes through the glomerular capillaries. Afferent arterioles bring blood in and efferent arterioles take blood out of the glomerulus. The glomerular capillaries are narrower than afferent arterioles. Ultra filtration happens when the pressure in the glomerular capillaries becomes very high. This happens continuously through semi permeable glomerular capillaries. Water and all substances dissolved in the blood plasma (except blood cells, colloids and certain plasma proteins) gets filtered into the Bowman’s capsule from the glomerular capillaries. Hence ultrafiltration is also called glomerular filtration. The filtrate fluid is called nephric filtrate, glomerular filtrate or ultrafiltrate. Hence the correct option is b.
3. Match the following column A with B. Column A has the parts of nephron and column B has the materials reabsorbed by the parts.
|
Column A |
Column B |
|
I) Ascending limb of Henle’s loop |
i) Water |
|
II) Descending limb of Henle’s loop |
ii) Electrolytes |
|
III) DCT |
iii) Na+ ions and HCO3- |
- I - i, II - ii, III - iii
- I - ii, II - i, III - iii
- I - iiii, II - i, III - ii
- I - i, II - iii, III - ii
Solution: Henle’s loop has a descending limb, and an ascending limb. The reabsorption process is different in both the loops. The descending limb of the loop of Henle is permeable to water but almost impermeable to electrolytes due to lack of transporters. The ascending limb is impermeable to water but allows transport of electrolytes actively or passively, because they lack aquaporins. Reabsorption of water, Na+ ions, HCO3- and amino acids occurs at DCT or distal convoluted tubule. Hence the correct option is b.
4. Which of the following are involved in the countercurrent mechanism for concentration of nephric filtrate?
- Henle’s loop and vasa recta
- PCT and vasa recta
- PCT and DCT
- Ascending loop of Henle and vasa recta
Solution: The urine is concentrated in Henle’s loop and vasa recta. The capillary network which forms a parallel set of hairpin loops within the medulla of kidney and supplies blood to it is called vasa recta. Blood flows in the opposite directions though the two limbs of Henle’s loop and this is same as in vasa recta. This forms a counter current pattern. This system of flowing a liquid in two limbs in opposite directions is termed as a countercurrent mechanism. The high solute concentration in the kidney medulla is maintained through this process. Hence the correct option is a.
FAQs
1. What is polyuria?
Answer: The abnormally large production or excessive formation of urine is called polyuria. The amount of urine will be greater than 2.5 L or 3 L in this case.
2. What are uricotelic animals?
Answer: Those animals which excrete uric acid as their nitrogenous waste are called uricotelic animals. Examples include insects, lizards, snakes, birds etc.
3. What is the colour of the urine in a patient with kidney failure?
Answer: One of the signs of kidney disease or failure is the light brown or tea coloured urine.
4. Why do we urinate more during winter?
Answer: The surrounding temperature is very low during winter. Hence the sweating will be less and there is no perspiration. Thus the kidney takes the entire process of excretion which results in more urine production.
YOUTUBE LINK: https://www.youtube.com/watch?v=3daW7mJaepg