-
Call Now
1800-102-2727


Transport of Gases, Oxygen Dissociation Curve, Practice Problems and FAQs
How often have you seen in space adventure movies that astronauts keep tracking the amount of available oxygen in their cylinders whenever they are out for a mission into outer space? Pretty much all space movies have a similar sequence and to be honest this is one of the crucial requirements to keep astronauts alive in space, even in reality. Do you know why? This is because earth is the only planet which has a high concentration of oxygen in its atmosphere which can support life, and we humans cannot survive without oxygen. Wonder why?
This is because we need oxygen to respire and produce energy in the cells. Without oxygen, our cells will not generate energy and will not be able to carry out any vital functions that are needed to keep us alive. Thus, oxygen is used by each and every cell of our body to oxidise glucose and generate energy. But how does oxygen in the air reach our cells? In fact, while we respire, we also generate carbon dioxide as a waste. So how do we get rid of the carbon dioxide?
You must be aware of the process of breathing, right? Breathing in helps us to take in the oxygen rich air into the lungs and breathing out helps us to get rid of the air rich in carbon dioxide from the body. The lungs help us in this process. But how is oxygen from the lungs taken to the cells or carbon dioxide from the cells taken to the lungs?
This is mediated by the circulating fluid in our body known as blood. In this article we are going to discuss about the transport of respiratory gases via blood in our body. Keep reading!
Table of contents
- Transport of gases in blood medium
- Transport of oxygen
- Oxygen- Haemoglobin Dissociation Curve
- Transport of carbon dioxide
External and internal respiration
Blood is the means of transport for O2 and CO2. Once the oxygen that we breathe in, reaches the alveoli of the lungs, it diffuses across the respiratory membrane (formed of alveolar wall, basement membrane and capillary wall) and enters the bloodstream of the capillaries surrounding the alveoli. Simultaneously, the carbon dioxide from the deoxygenated blood, that was brought to the lungs, diffuses out of the capillaries and crosses the respiratory membrane to reach the alveoli. It is exhaled out. This exchange of gases between the lungs and the atmospheric air is known as external respiration.

Fig: External respiration
The oxygen that diffuses into the blood is then transported to the tissues where it diffuses into the cells of the tissues and carbon dioxide generated by the cells as a result of cellular respiration diffuses into the blood to be carried back to the lungs to be expelled out. This exchange of gases between the blood and the tissues is known as internal respiration.

Fig: Internal respiration
Both CO2 and O2 are transported through the blood medium.The mechanisms associated with transport of these two gases are different.
Transport of oxygen
About 4.6 ml oxygen enters each 100 ml of blood in alveolar capillaries of lungs during external respiration. It is transported to the tissues of the body by blood in two forms -
- About 97 percent of oxygen diffuses into the RBCs and binds with the ferrous ions present in the haemoglobin of RBC to form oxyhaemoglobin.
- The remaining 3 percent of oxygen is transported through the plasma in a dissolved state.
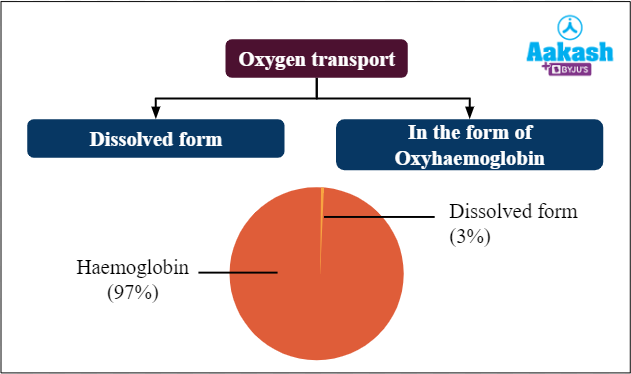
Fig: Transport of oxygen
Transport of Oxygen in dissolved form in Plasma
The blood plasma is the liquid component of blood which has oxygen in a dissolved state (3%). However, oxygen is not completely soluble in blood as a result of which only 3% is transported in this form.
Transport of Oxygen in the form of Oxyhaemoglobin
The Red blood cells have a respiratory pigment called haemoglobin which binds with oxygen to form oxyhaemoglobin.
Haemoglobin
The haemoglobin is made up of globin and haem units. Globin is the protein part and haem is the red iron porphyrin ring that gives red colour to the blood. There are 4 protein chains - Two alpha and two beta chains along with 4 haems. Each haem has an iron ion in the ferrous state (Fe2+) at its centre.

Fig: Structure of haemoglobin
Each ferrous ion can bind with one molecule of oxygen and oxidise into ferric ions (Fe3+). Thus, each molecule of oxyhaemoglobin can carry a maximum of four molecules of oxygen.

Fig: Formation of oxyhaemoglobin
Loading and unloading of haemoglobin
Oxygenation of haemoglobin to form oxyhaemoglobin is known as the loading reaction. In pulmonary alveoli, the partial pressure of oxygen (pO2) is high and partial pressure of carbon dioxide (pCO2) is low, whereas in capillary blood the pO2 is less and pCO2 is high. Partial pressure is the pressure exerted by individual gases in a mixture. Higher the concentration of a gas in a mixture, greater is its partial pressure. Gases tend to diffuse from a region of higher partial pressure to a region of lower partial pressure. Thus, O2 from the pulmonary alveoli diffuses into the blood capillaries and binds with haemoglobin present in the RBCs of blood, Affinity of haemoglobin towards oxygen increases with the fall of pCO2 of the blood as CO2 from the capillary blood diffuses into the alveolar air during gaseous exchange.
In the tissue capillaries, oxyhaemoglobin breaks down to form haemoglobin and molecular oxygen. This is known as the unloading reaction. This reduced form of haemoglobin is known as deoxyhaemoglobin. In an active tissue, cells are continuously performing cellular respiration and hence pO2 is much lower and pCO2 is much higher. At high pCO2. The affinity of haemoglobin towards oxygen reduces and more oxyhaemoglobin dissociates.

Fig: Loading and unloading of haemoglobin
Oxygen carrying capacity of blood
The oxygen carrying capacity of blood depends on the concentration of haemoglobin. Blood has 14.5 to 15 g of haemoglobin in every 100 ml. When fully saturated, 1 gm of haemoglobin binds with 1.34 ml of oxygen. Thus, every 100 ml of blood can carry approx 19.43 - 20.1 ml of oxygen.
Oxyhaemoglobin Dissociation Curve
The blood in the capillaries that is brought by the arteries (arterial blood) has 97% oxyhaemoglobin whereas the blood in the capillaries that is about to leave via the veins (venous blood) has about 75% oxyhaemoglobin saturation. This indicates that the blood entering the tissues contains around 20 ml of oxygen per 100 ml of blood, whereas the blood leaving the tissues contains only 14 ml of oxygen per 100 ml of blood. Thus, around 5 - 6 ml of the 20 ml of oxygen brought to the tissues, by every 100 ml of blood, is unloaded to the tissues. A graph plotted to depict the saturation percentage of oxyhaemoglobin and partial pressure of oxygen is known as the Oxyhaemoglobin Dissociation Curve. It was constructed by J.S. Haldane in 1898.
|
|
Arterial blood |
Venous blood |
|
Oxyhaemoglobin percentage |
97% |
75% |
|
pO2 |
95 mm Hg |
40 mm Hg |
|
Oxygen content |
19-20 ml per 100 ml blood |
14 ml per 100 ml blood |
In alveoli there is high pO2, low pCO2, less H+ and less temperature. All these factors are in favour of oxyhaemoglobin in association. In tissues, low pO2, high pCO2, high H+ and high temperature are in favour dissociation of O2 from oxyhaemoglobin. The oxygen - haemoglobin curve also known as oxygen dissociation curve is sigmoid or S shaped. At high pO2 values the curve is relatively flat whereas it becomes very steep at lower pO2 values. The S shaped curve is seen only under normal conditions. As the conditions change, the pattern of the curve also varies.

Fig: Oxygen Dissociation curve
Changes in pO2 at high pO2 values such as 80 and above, have very little effect on the loading and unloading reaction and on the oxygen content of blood. Changes in pO2 at 50 mm Hg or less, where the curve is very steep, the dissociation of oxyhaemoglobin is very rapid. This is what happens at the tissues which have high pCO2 and low pO2 and hence unloading of oxyhaemoglobin occurs rapidly. In the lungs, uptake of oxygen by reduced haemoglobin in the deoxygenated blood occurs rapidly.
Factors affecting Oxygen dissociation curve
There are multiple factors which influence the dissociation of oxyhaemoglobin to release oxygen. These are -
Partial pressure of oxygen
As the partial pressure of oxygen increases, the affinity of haemoglobin towards O2 also increases.
Partial pressure of carbon dioxide
As the partial pressure of carbon dioxide in the blood increases, the affinity of haemoglobin towards O2 decreases.
Temperature
At higher temperatures, the bond between oxygen and haemoglobin weakens and dissociation of oxyhaemoglobin is more rapid. Thus, at higher temperature more oxygen is unloaded to the tissues.
pH or H+ ion concentration
Upon its release in the blood, carbon dioxide reacts with water in the blood to form carbonic acid. It then dissociates into hydrogen ions and bicarbonate ions.
Fig: Formation and dissociation of carbonic acid
As the release of H+ ions increases with increase in carbon dioxide concentration (pCO2) in blood, the blood becomes more acidic and its pH is reduced. At a pH lower than 7.4 (normal pH of blood), the affinity of haemoglobin towards oxygen is reduced and it dissociates rapidly. This occurs when CO2 from the tissues is released into the blood and thus, rapid dissociation of oxyhaemoglobin occurs at the tissues to rapidly deliver oxygen to them. Decreased affinity of haemoglobin towards O2 and rapid dissociation of oxyhaemoglobin shifts the oxygen dissociation curve to the left.

Fig: Left shift of oxygen dissociation curve due to low blood pH
At pH higher than normal pH of blood, the affinity of haemoglobin towards oxygen is increased and dissociation is reduced. This causes the shift of the oxygen dissociation curve to the right. This occurs when there is less carbon dioxide released into the blood which results in less concentration of H+ ions in the blood and hence higher pH.

Fig: Right shift of oxygen dissociation curve due to high blood pH
Bohr effect
The phenomenon of increase in carbon dioxide concentration leading to increased dissociation of oxyhaemoglobin to release more oxygen is known as Bohr effect. According to the Bohr effect, the affinity of haemoglobin towards oxygen is reduced when pH is lower than normal blood pH and increased when pH is higher than normal blood pH. It plays a crucial role in oxygenation of blood in lungs and release of oxygen in tissues.
Transport of carbon dioxide
There are 3 ways in which CO2 is transported in the blood.

Fig: Transport of carbon dioxide
Transport of CO2 in the form of Carbaminohaemoglobin
Around 30% of the carbon dioxide entering the RBCs, enters into a loose combination with the globin part of deoxyhemoglobin (reduced haemoglobin) to form carbaminohemoglobin. Four molecules CO2 molecules bind to the amine groups on the protein chains of the globin part of haemoglobin..

Fig: Carbaminohaemoglobin
Transport of CO2 dissolved in plasma
Carbon dioxide is around 20-25 times more soluble than oxygen in water. Therefore 7% of total carbon dioxide present in blood dissolves in the blood plasma and is carried as a simple physical solution.
Transport of CO2 in the form of bicarbonates
Around 70% of the carbon dioxide diffuses into RBCs and combines with water to form carbonic acid. This reaction is catalysed by the enzyme carbonic anhydrase. Being unstable, carbonic acid quickly dissociates into bicarbonate ions and hydrogen ions.
This enzyme reversibly catalyses the conversion of carbon dioxide and water to carbonic acid. The H+ ions are picked up by proteins and only a small percentage of the bicarbonate ions are transported via the RBCs. The rest come out into the blood plasma and combine with metallic ions to form metal bicarbonates and are transported as soluble salts.
When bicarbonate ions from RBC move into plasma the ionic balance between plasma and RBC is altered. Chloride ions from plasma diffuse into RBC in order to restore the ionic balance. This movement of chloride ions is known as chloride shift or Hamburger’s phenomenon.

Fig: Transport of carbon dioxide as bicarbonate ions
Release of carbon dioxide in alveoli
The venous blood leaving the tissues is rich in carbon dioxide and is taken to the lungs for oxygenation. Upon reaching the lungs, due to high pO2 in the alveoli, the oxygen readily diffuses into blood and associates with haemoglobin to form oxyhaemoglobin. Simultaneously, carbon dioxide is also released because oxyhaemoglobin is a stronger acid than deoxyhemoglobin and releases H+ ions which combine with bicarbonate ions in the blood to form carbonic acid. Carbonic anhydrase breaks down the carbonic acid to form water and carbon dioxide and thus, carbon dioxide is released from bicarbonate. The pCO2 being high in the blood and low in the alveoli, carbon dioxide diffuses out into the lungs to be expelled out.
Oxygenation of haemoglobin also releases carbon dioxide from carbamino haemoglobin because oxyhaemoglobin cannot hold as much carbon dioxide as deoxyhaemoglobin can.
Haldane effect
The phenomenon of displacement of carbon dioxide from carbaminohemoglobin due to formation of oxyhaemoglobin is known as the Haldane effect.
Practice problems
Q1. Due to which of the following factors the oxygen dissociation curve will shift to the right?
A. High pH
B. High pCO2
C. Low temperature
D. High pO2
Solution: The oxygen dissociation curve shifts to the right when the affinity of haemoglobin towards oxygen is reduced and the dissociation of oxyhaemoglobin increases. pH higher than the normal pH of blood, low temperature and high pO2 increase the affinity between haemoglobin and oxygen and hence reduce dissociation of oxyhaemoglobin. Thus, these factors shift the curve to the left. But high pCO2 promotes dissociation of oxyhaemoglobin and shifts the curve to the right.
Thus, the correct option is b.
Q2. Majority of carbon dioxide (CO2) released into the blood, from the tissues, is present as
A. carbaminohemoglobin in plasma
B. dissolved in a physical solution in plasma
C. carbaminohaemoglobin in erythrocytes
D. bicarbonate in blood plasma and erythrocytes
Solution: There are 3 ways in which CO2 is transported in the blood.

Fig: Transport of carbon dioxide
Around 7% of carbon dioxide dissolves in plasma and is transported as physical solution. 30% combines with haemoglobin in erythrocytes and is transported as carbamino haemoglobin. Around 70% of carbon dioxide enters the erythrocytes and combine with water to form carbonic acid. The carbonic acid dissociates into H+ ions and bicarbonate ions. A small percentage of the bicarbonate ions are transported via the erythrocytes and the majority leak into the plasma to combine with metallic ions to metallic bicarbonates and are transported in this form.
Thus, the correct option is a.
Q3. Find the correct statement.
A. The partial pressure of oxygen is high in tissues and low in alveoli
B. The partial pressure of carbon dioxide is high in alveoli and low in tissues
C. The partial pressure of oxygen is high in alveoli and low in active tissues
D. The partial pressure of carbon dioxide is high in the tissue capillaries and low in the intercellular fluid
Solution: The partial pressure of oxygen is high in the alveoli compared to that in the alveolar capillary. Thus oxygen from the alveoli diffuses into the blood in the alveolar capillary.
In the tissues, cellular respiration generates a lot of carbon dioxide. Thus, partial pressure of carbon dioxide in the intercellular fluid of tissues is higher compared to the arterial blood that is brought to them via the capillaries. Thus, carbon dioxide diffuses from the tissues into the blood and makes the blood venous. As active tissues use up a lot of oxygen to release carbon dioxide via cellular respiration, the pO2 in active tissues is quite less compared to arterial blood in the capillaries. Thus, oxygen from the blood diffuses into the cells in the tissues.
In the lungs, the blood present in the capillaries surrounding the alveoli is venous and has high pCO2 compared to air in alveoli. Thus carbon dioxide from the capillaries diffuses into the alveoli to be exhaled out.
Thus, the correct option is c.
Q4. Chloride shift is the
A. Movement of chloride ions from the plasma into the RBCs
B. Movement of chloride ions from RBCs into plasma
C. Movement of chloride ions from plasma into interstitial or intercellular fluid
D. Movement of chloride ions from interstitial or intercellular fluid into plasma
Solution: Around 70% of carbon dioxide enters the erythrocytes and combine with water to form carbonic acid. The carbonic acid dissociates into H+ ions and bicarbonate ions. A small percentage of the bicarbonate ions are transported via the erythrocytes and the majority leak into the plasma to combine with metallic ions to metallic bicarbonates and are transported in this form.
When bicarbonate ions from RBC move into plasma the ionic balance between plasma and RBC is altered. Chloride ions from plasma diffuse into RBC in order to restore the ionic balance. This movement of chloride ions is known as chloride shift or Hamburger’s phenomenon.
Thus, the correct option is a.
FAQs
Question 1. What is Polycythemia?
Answer: Polycythemia is a condition in which the volume percentage of red blood cells in blood increases abnormally.
Question 2. What is hypoxia?
Answer: Hypoxia is a condition in which the the level of oxygen in body tissues becomes very less. Hypoxia can result in mental confusion, restlessness, laboured breathing, increased heart rate, and bluish skin.
Question 3. What happens when we breathe in high concentration of carbon monoxide?
Answer: Carbon monoxide is highly toxic when inhaled in high concentration because it forms an irreversible combination with haemoglobin to form carboxyhaemoglobin which cannot be dissociated. Thus, as the individual breathes in more and more carbon monoxide, an increasing number of haemoglobin molecules get converted into carboxyhaemoglobin and are not available for transporting oxygen to the tissues. This can lead to hypoxia and eventually kill the person.
Question 4. Why can’t we breathe underwater?
Answer: We cannot breathe under water because our lungs are not designed to break down water and release oxygen as the process requires a lot of oxygen. Extraction of dissolved oxygen from water is not easy as density of water is much higher than the density of air and our lungs cannot filter separate oxygen from water.
YOUTUBE VIDEO:
Related Topics
|
Mechanism of breathing, Difference between inspiration and expiration, Abdominal breathing, Thoracic breathing, Hering - Breuer reflex |
|
Respiration - Introduction, Respiratory organs in animals |
|
Lung Volumes and Capacities |
|
Exchange of gases: Partial pressure, Diffusion, Sites of exchange of gases |
|
Regulation of Respiration |
|
Disorders of the Respiratory System: Mountain sickness, Chronic obstructive pulmonary disease, Bronchial asthma, Pulmonary tuberculosis, Pneumonia, Occupational respiratory disorders, Severe acute respiratory syndrome |
|
Human Respiratory System: Respiratory Tract, Structure of Lungs |